
Introduction
The meibomian glands are specialized sebaceous glands located within the tarsal plates of the eyelids. They play a critical role in ocular health by secreting meibum, a lipid-rich substance that prevents tear evaporation and maintains the stability of the tear film. When these glands become obstructed, the resulting inflammation can lead to the formation of a chalazion—a chronic, sterile, lipogranulomatous lesion. Understanding the distinction between incision and drainage (I&D) and complete surgical excision is essential for clinicians aiming to balance effective lesion resolution with long-term ocular surface preservation.
The pathophysiology of these lesions often involves chronic meibomian gland dysfunction (MGD), where altered lipid composition leads to ductal stasis. If left unmanaged, the resulting granulomatous response can impact the ocular surface, causing discomfort, blurred vision, and chronic irritation.
Clinical Evaluation
Accurate diagnosis is the cornerstone of successful management. Clinicians must differentiate between a simple chalazion, an acute hordeolum (stye), and more concerning pathologies such as sebaceous gland carcinoma. A thorough history should assess the duration of the lesion, previous recurrences, and any associated systemic conditions. Physical examination should focus on the lid margin, the character of the meibum, and the presence of any lash loss or atypical vascularization, which may necessitate a biopsy to rule out malignancy.
Surgical Treatment Options
Incision and Drainage (Incision & Curettage)
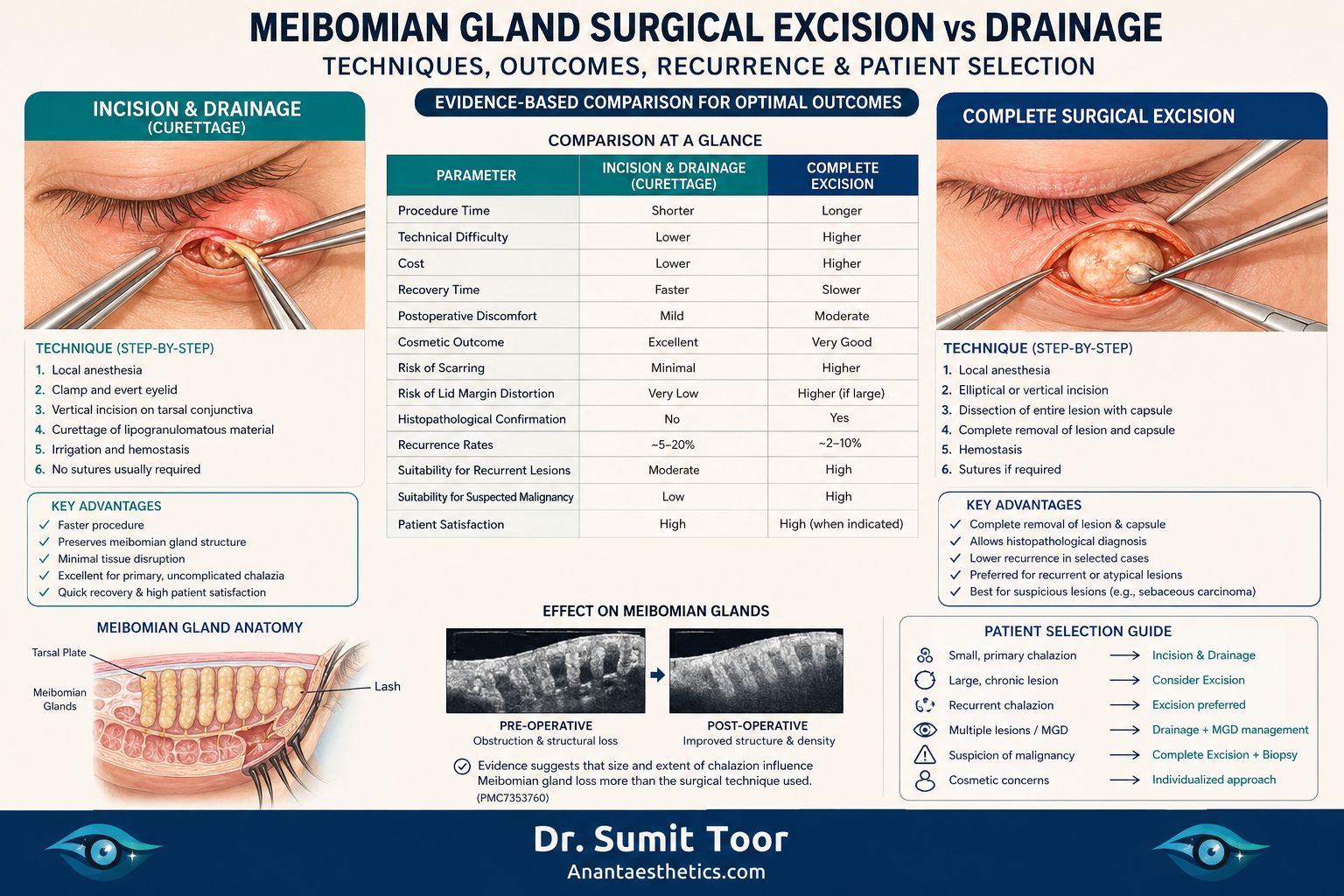
Incision and curettage remains the gold standard for persistent, uncomplicated chalazia. The procedure involves local anesthesia, followed by the application of a chalazion clamp to provide hemostasis and stabilization. A vertical or horizontal incision is made through the conjunctiva (or skin, depending on the lesion's location), and the contents are curetted. This technique is favored for its speed, minimal tissue disruption, and high success rate in primary cases.
Complete Surgical Excision
Complete excision involves the removal of the entire lesion, including its fibrous capsule. This approach is indicated for recurrent lesions, atypical presentations, or when there is a high index of suspicion for malignancy. Unlike simple drainage, this method provides a tissue specimen for histopathological examination, which is vital for definitive diagnosis.
Comparative Analysis
| Feature | Incision & Drainage | Complete Excision |
|---|---|---|
| Technical Difficulty | Low | Moderate to High |
| Histopathology | Limited | Comprehensive |
| Recurrence Risk | Moderate | Lower |
| Cosmetic Outcome | Excellent | Variable (requires closure) |
Outcomes and Evidence Review
Current literature suggests that meibomian gland loss is more closely correlated with the size and duration of the chalazion itself rather than the surgical technique employed. Studies have demonstrated that successful drainage can actually improve meibomian gland morphology and tear film stability by relieving the pressure on surrounding healthy glands. While complete excision offers a lower recurrence rate for chronic, fibrotic lesions, it requires more meticulous surgical planning to avoid lid margin distortion.
- Standard Treatment: Incision and curettage remains the standard treatment for persistent chalazion and has been shown to improve meibomian gland morphology and ocular surface parameters after surgery.
- Gland Loss Correlation: Available studies suggest that meibomian gland loss is more closely related to the size and extent of the chalazion itself than to whether surgery or conservative treatment is used.
- Value of Excision: Complete excision is particularly valuable for recurrent, atypical, or suspicious lesions because it allows full histopathological evaluation.
Patient Selection Algorithm
-
1Small Primary Lesion Incision and drainage is the recommended first-line approach.
-
2Large / Chronic Lesion Consider complete excision if the capsule is thick, fibrotic, or non-responsive.
-
3Recurrent / Atypical Lesion Complete excision with mandatory histopathology to rule out underlying conditions.
-
4Suspicion of Malignancy Complete surgical excision is mandatory for definitive diagnosis.
Expert Recommendations
Incision and drainage should remain the first-line treatment for the majority of chalazia. Complete excision should be reserved for cases where the lesion is recurrent, atypical, or where malignancy cannot be ruled out. Individualized care, focusing on the preservation of the meibomian gland architecture, is paramount for long-term ocular surface health.
Anant Aesthetic Clinic, located in Adampur, is a premier center for advanced aesthetic and oculoplastic care. Led by Dr. Sumit Toor and Dr. Pratibha Toor, the clinic is dedicated to providing evidence-based, patient-centered treatments. With a focus on precision and natural-looking results, the team at Anant Aesthetic Clinic combines clinical expertise with a compassionate approach to ensure the highest standards of care for every patient.